
Micronutrient therapy
| Definition | |
|
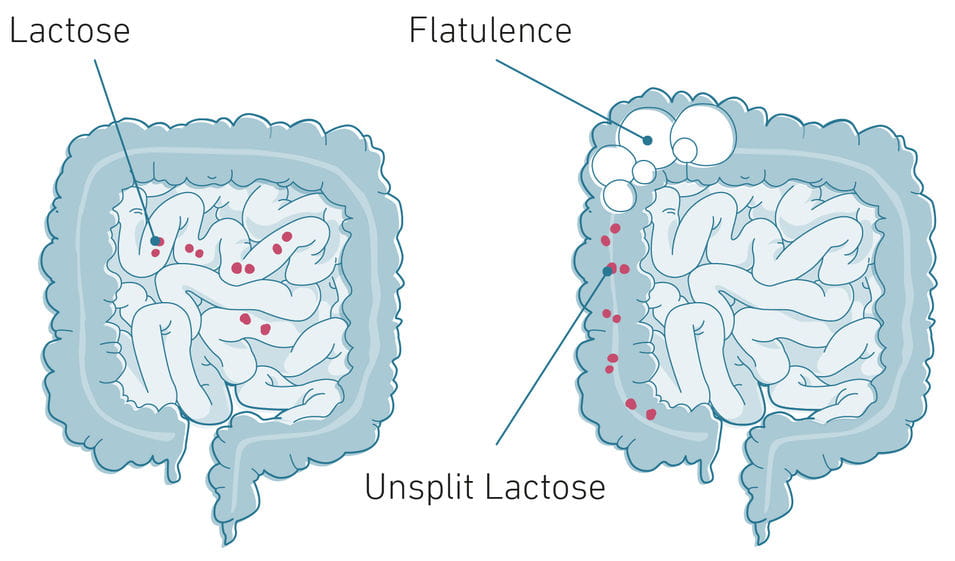
Lactose intolerance refers to incomplete digestion of milk sugar (lactose) in food due to a reduced or absent production of the digestive enzyme lactase. Worldwide about 70–75 % of the population cannot fully utilize lactose after infancy, only a few populations maintain lactase activity into adulthood. The enzyme lactase is formed in all healthy newborns in the mucous membrane of the small intestine and splits the disaccharide lactose into the monosaccharides D-glucose and D-galactose, which are then absorbed into the blood. With natural weaning from breast milk, lactase activity also drops to about 5–10 %. Only in populations with a long history of dairy farming and animal breeding have persistent lactase production into adulthood. If lactase activity is limited or absent, the unsplit lactose reaches the large intestine, where it is fermented by intestinal bacteria. The resulting fermentation products lactate, methane and hydrogen subsequently lead to flatulence and diarrhea. The cause of a lactase deficiency is either congenital or acquired in the natural course of life. However, lactose intolerance differs fundamentally from a milk protein allergy, which is IgE antibody-mediated and represents an active immune response. |
|
| Symptoms | |
|
In lactose intolerant people, the lactose, which is mainly absorbed from milk and milk products, is incompletely broken down in the small intestine and reaches the large intestine, where the intestinal bacteria ferment it. As a result of the misdirected utilization, gases and organic acids are produced which lead to flatulence, abdominal pressure, cramps, nausea, vomiting and diarrhea. In addition, non-specific symptoms such as headaches, chronic fatigue, restlessness, tachycardia, increased blood pressure, vertigo, headaches, outbreaks of sweating, feelings of exhaustion, sleep disorders, concentration disorders and acne can also occur. Lactase activity may be mild or completely absent which correlated to the severity of the symptoms. It should be noted that the symptoms of congenital lactose intolerance are much more severe than those of adult lactose intolerance. The irritation of the intestinal mucosa associated with lactose intolerance leads to diarrhea, which can disrupt the absorption of vitamins, minerals and trace elements. Long-term diarrhea can even lead to a curvature of the intestinal villi, which reduces the absorption of all nutrients.
|
|
| Causes | |
|
The cause of lactase deficiency includes variety of factors. In congenital lactase deficiency (congenital lactase deficiency, CLD) the enzyme is severely restricted or not formed at all due to a genetic defect. This form is a rare autosomal recessive hereditary disease which has been described in the Finnish population and leads to diarrhea in the first days after birth and severe brain damage in the newborn. A developmental lactase deficiency is a rare form that can occur in premature babies. Due to the late formation of lactase in the last weeks of pregnancy, preterm babies are often unable to process lactose. This form of lactase deficiency is not deterministic of lactose tolerance in adulthood. In primary lactose intolerance – the world's most common form – lactase production in the small intestine of infants is sufficient but decreases after weaning. In the majority of cases, enzyme activity is lost from around the age of five. As a rule, lactase activity does not decrease completely, but shows a certain inducibility with continuous exposue to lactose. The genetic predisposition for this form of lactose intolerance can be determined by the LCT genotype. Adults in northern regions often have no problems with lactose intake into old age. The reason for the persistence of enzyme production in adulthood is an inherited mutation.Triggers for secondary lactose intolerance according to Leiß et al. 2005, includes chronic intestinal diseases, intestinal lymphoma, bacterial or viral gastroenteritis, partial or total gastrectomy, short bowel syndrome, malnutrition, blind sack syndrome/large duodenal diverticulum, chemotherapy/radiation therapy, chronic alcohol abuse and small bowel parasites from the group of giardiasis. In addition, diseases of the digestive system can also damage the lactase-producing cells to such an extent that lactase production is temporarily impaired, and in rare cases even for life. |
| Diagnosis | ||||||||||||||
|
There are various examination options available for the diagnosis of lactose intolerance. The common H2-breath test is based on the detection of hydrogen (H2) in exhaled breath and serves as indirect detection of lactase deficiency. During the bacterial processing of the lactose in the large intestine, lactic acid, acetic acid, carbon dioxide and gaseous hydrogen is produced in the affected individuals, which enters the lungs via the blood and is breathed out. Since under normal circumstances there is no hydrogen in the exhaled air, a positive result may indicate lactose intolerance. This test measures the concentration of hydrogen before and after oral administration of a certain amount of lactose. If the measurement result before and after lactose administration differs by 20 ppm, the result is positive. However, this test leads to a false negative result in every fifth patient, since a disturbed intestinal flora (harmless) may also contain lactose-utilizing bacteria. In addition, a gene test for the LCT genotype is available, which only requires a cheek swab. By assigning the LCT genotype to TT, TC or CC (lactose intolerance) the genetic predisposition of the patient can be determined. In exceptional cases, a tissue sample can also be taken from the small intestine and the lactase activity in the small intestine tissue can be examined. In addition, potential lactose intolerance may also be detected by a diet or exposure test. In the diet test the affected person avoids lactose-containing milk products for several days, including lactose which is added to processed products. If no symptoms occur during this period, lactose intolerance may be present. In a exposure test the affected person drinks a glass with about 50–100 g dissolved lactose after a few days of lactose avoidance. If the typical symptoms appear within a few hours, lactose intolerance can be assumed. However, a doctor should be consulted for a complete diagnosis. |
||||||||||||||
| Therapy | ||||||||||||||
|
Since the symptoms of lactose intolerance are due to the lactose, the main focus of therapy – depending on the severity of the intolerance – is on reducing or avoiding products containing lactose.
In the case of lactose intolerance, it is the unused sugar content that changes the bacterial composition in the intestine and leads to complaints. In cases of mild intolerance, many sufferers usually tolerate small amounts of lactose without symptoms, which is why complete avoidance of lactose is not often necessary. However, in the case of moderate and severe forms of lactose intolerance, an elimination diet is recommended in which not only the lactose itself but also malabsorbed carbohydrates such as fructose (fructose), sorbitol, xylitol and other sugars should be avoided. In addition, it is advisable to avoid beans, leeks, and cabbage during the first weeks of treatment, as well as taking resorption inhibiting medication and non-resorbable sugars. All other fiber types also change the bacterial intestinal flora through the increased formation of short-chain fatty acids, CO2 and other biogenic amines, so that these should be avoided at least in the initial phase of elimination. Milk has a lactose content of about 4.8 % and thus has the highest lactose content. The lactose content of milk products varies greatly depending on the method of production. For example, in the production of some types of cheese, buttermilk and yoghurt, bacteria are used that break down lactose by fermentation, which is why the end product can be lactose-free. However, in order to ensure a longer shelf life of food, the processing interrupts the fermentation process at an early stage, which is why many yoghurts and kefirs are not lactose-free. For cheese in general, the longer the maturing process, the lower the lactose content. In this context, however, it should also be mentioned that biogenic amines are formed during a long ripening period, which can lead to pseudoallergies, the physiological effects of which can be just as unpleasant as histamine in a real allergy. There is now a large selection of lactose-free milk and dairy products on the market. For this purpose, lactose is almost completely removed by enzymatic splitting. Those affected must also pay attention to the addition of lactose in finished products and medicines. Another possible remedy is to take the enzyme lactase in capsule or tablet form as needed, whereby the exact dosage must be adapted to the food to be consumed and the individual tolerance threshold. Milk substitutes such as soy, almond and cereal drinks are also a good alternative as they are often enriched with vitamins and calcium. Whether the avoidance of milk and dairy products leads to nutrient deficiencies, especially calcium deficiency, depends on dietary habits. Since milk and dairy products are important sources of calcium, people with lactose intolerance can resort to other valuable calcium sources such as calcium-containing mineral water (150 mg calcium per liter). In addition, some vegetables, such as broccoli and kale, have a high calcium content. In addition, foods enriched with calcium (e.g. some fruit juices) can be increasingly integrated into the diet. Regular monitoring of the calcium level in the blood is a sensible measure for the prevention of osteoporosis in a milk and milk product-free diet. If the lactose intolerance has arisen in the course of a disease of the digestive system, a complete disappearance of the lactase deficiency can be assumed after the treatment of the disease. Only in rare cases are the damages of the lactase-producing tissue so severe that it no longer recovers.
|
| Relevant micronutrients | |
|
To promote digestive performance in cases of lactose intolerance, it is advisable to administer a targeted, timely lactase replacement preparation that increases the capacity for enzymatic lactic acid cleavage and reduces undesired symptoms. Zinc and vitamin C are closely associated with immune and healing processes and promote the restoration of healthy intestinal mucosa. Green tea extract can reduce the permeability of the intestinal mucosa andprevent the penetration of antigens and pathogenic germs due to its astringent effect. The constituent epigallocatechin-3-gallate acts as a strong electron donor and is an effective antioxidant in the inflammatory process. These effects have been demonstrated both in the small intestine and in the large intestine. Chamomile extract strengthens the healing process through its antiphlogistic and granulation-promoting properties. L-Glutamine plays a central role in the formation and maintenance of cell systems. Cells with high division rates, such as the cells of the immune system and the mucosa cells of the small intestine, depend on a sufficient supply of the amino acid glutamine. In addition, L-glutamine as a precursor of glutathione biosynthesis is a central component for maintaining the antioxidative status. In the prevention of food allergies, probiotic microorganisms appear to play an important role. Stimulation of the intestinal immune system (GALT) activates the immune defense and stimulates immune cell proliferation, cytokine release and antibody production. |