Micronutrient therapy
| Definition |
|
The female menstrual cycle is a repetitive process that occurs up to 400 times in a woman's life. The entire cycle is characterized by hormonal changes, some of which have an effect on physical well-being and mood. Premenstrual Syndrome (PMS) is a complex of everyday disturbances that occur mainly in the second half of the cycle and are associated with some mild but severe symptoms. Physical complaints such as water retention in the tissues, abdominal pain and breakouts are often accompanied by psychological complaints such as fatigue, irritability and feelings of depression. Many women suffer from PMS symptoms to varying degrees. It is estimated that three quarters of women of childbearing age are affected, mainly between 30 and 40 years of age. Of these, 3-8% suffer from a particularly severe form of PMS, premenstrual dysphoric disorder (PMDS). |
| Symptoms |
|
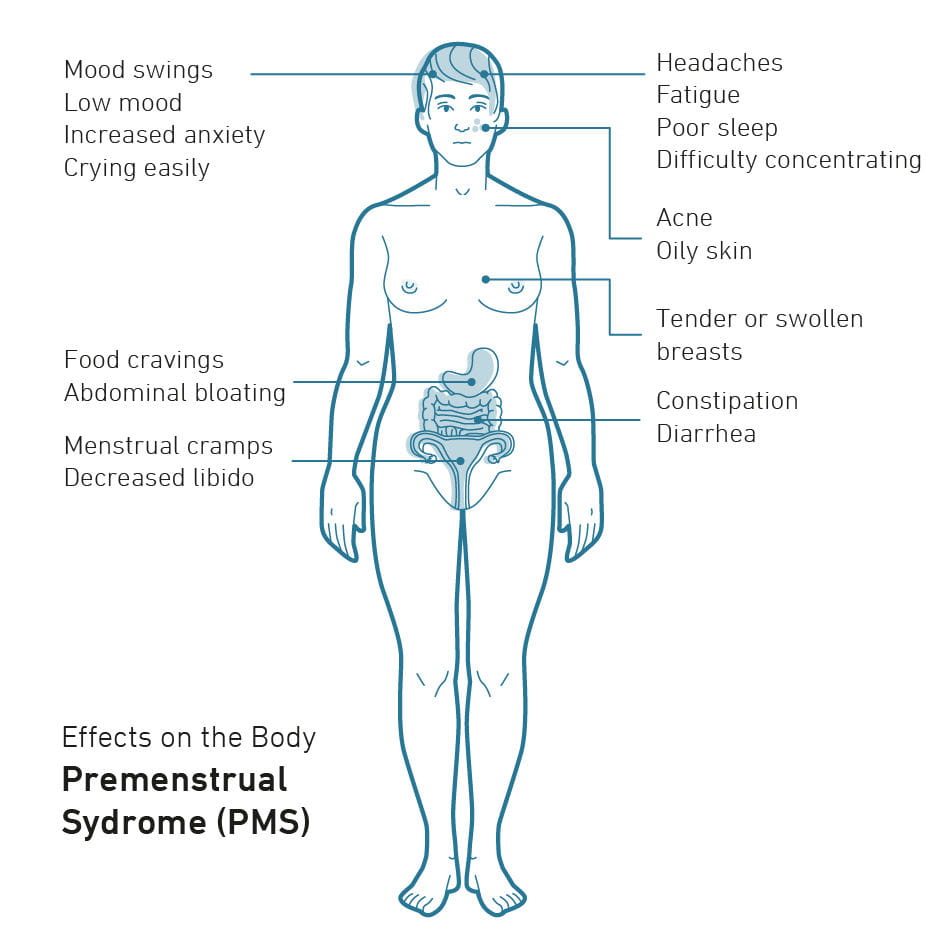
PMS occurs after ovulation in the second phase of the cycle and can last for either a few days or up to 2 weeks. As a rule, the symptoms subside in most patients with the onset of menstrual bleeding. The symptoms and severity of PMS vary from woman to woman. While some women complain of a few symptoms on a few days, others find the entire second half of the cycle very stressful. Physical symptoms include marked tiredness, symptoms of fatigue, feeling unwell, abdominal cramps, gastrointestinal complaints, skin changes, circulatory problems, water retention in the body, backache, headaches and even migraines, sensitivity, swelling or tightness of the breasts, weight gain, fainting, increased sensitivity to stimuli and pain in the genital area. Psychological symptoms may also occur, including irritability, mood swings, aggression, feelings of overexertion and loss of control, listlessness, hyperactivity, restlessness, ravenous hunger or loss of appetite, anxiety, depressive or manic moods, and groundless laughter or crying. A small percentage of women are affected by a particularly severe form of mental stress. In the so-called premenstrual dysphoric disorder (PMDS), the symptoms of aggressiveness, anger, irritability, depression and anxiety are so strong that they have an effect on the professional, social and family environment.
|
| Causes |
| Despite many years of research, the exact causes of PMS have not yet been clarified, but a multifactorial cause is assumed. One of the possible causes of PMS is hormonal changes in the second half of the cycle after ovulation and the onset of menstrual bleeding. This includes a unbalance of the sex hormones progesterone and estrogen, as well as prolactin, which increases in the second half of the cycle. This hormonal change can then lead to the typical physical and psychological complaints of PMS in the body. Furthermore, a number of other factors can contribute to the worsening of premenstrual syndrome, including thyroid disorders, fluctuations in serotonin levels, prolonged stress, psychological stress, sleep disorders, unhealthy eating habits and excessive consumption of nicotine, caffeine and alcohol. |
| Diagnostics |
|
The first step is diagnosis is a detailed patient history.. A symptom diary can also help to give a more complete picture. In order to distinguish PMS from other illnesses with similar symptoms and to obtain a clear diagnosis, appropriate physical examinations as well as blood tests, including hormone status, are necessary. A basic PMS profile measures parameters such as estradiol and progesterone levels taken in the second half of the cycle. Ideally, progesterone should be determined between the 19th and 21st day of the cycle. Furthermore, a PMS Plus profile can be performed, in which further parameters such as calcium, folic acid, fT3 and fT4 (thyroid hormones), magnesium, prolactin, serotonin, TSH (hormone of the pituitary gland to regulate the formation of thyroid hormones), vitamin B6 as well as zinc in serum, EDTA blood or lithium heparin blood are examined. EDTA blood is blood which is made uncoagulable for Diagnostic tests with the chelating agent Ethylenediaminetetraacetic acid (EDTA). In heparin blood coagulation is counteracted with heparin (lithium heparinate). |
| Therapy |
|
To alleviate the symptoms of PMS, adapted micronutrient therapy and, if necessary, appropriate medication can be applied. Due to the complex interaction of the various causal mechanisms, therapy is primarily targeted toward symptoms However, a healthy lifestyle with regular physical activity, sufficient sleep and rest, a salt-reduced and healthy diet as well as the avoidance of coffee, nicotine and alcohol can in many cases significantly alleviate the symptoms in the second half of the cycle. |
| Relevant micronutrients |
|
Pyridoxal 5-phosphate (P5P, PLP), the metabolically active form of vitamin B6, not only has a role in the synthesis of prostaglandins and fatty acids, but is also important for the formation of neurotransmitters, such as dopamine and serotonin. It has already been scientifically demonstrated that vitamin B6 contributes to normal mental function and the regulation of hormonal activity. Use of oral contraceptives has been associated with nervousness, irritability and depression. It is known that the vitamin B6 levels of users of oral contraceptives are significantly lower than those of non-users – accordingly, a physiological relationship can be identified. Vitamin B6 in high doses has been successfully used in several studies to treat feelings of depression in the premenstrual phase. A beneficial effect on psychological symptoms – such as low moods, irritability and concentration difficulties – and general discomfort was shown. In addition, a lack of vitamin B6 is associated with increased water retention and premenstrual acne, which can be counteracted by the administration of vitamin B6. The effectiveness of vitamin B6 therapy on premenopausal women with hormone-dependent depression has also been demonstrated. In addition to the effects of vitamin-B6 on PMS, low doses of vitamin B1 and vitamin B2 are also associated with a reduced occurrence of PMS because these B vitamins are integrated into neurotransmitter metabolism via various mechanisms. Vitamin B6 is successfully used for painful menstrual bleeding and feelings of depression in the premenstrual phase. In several clinical studies, vitamin B6 supplementation could favorably influence both PMS and premenstrual depression. Deficiencies of calcium and magnesium are also associated with the occurrence of menstrual pain. In order to improve the uptake of the two minerals, vitamin D should also be supplemented. Women lose between 30 and 40 ml of blood per cycle; in the case of severe blood loss it can be as high as 60 to 80 ml. Even higher quantities are referred to as abnormal uterine bleeding or menorrhagia. Iron status is more affected if the blood loss is more than 60 ml. Iron deficiency leads to a reduced haemoglobin and erythrocyte concentration with unspecific symptoms and ultimately manifests in the form of anemia. Reduced oxygen transport in the blood impairs the supply of organs and tissues. This causes general symptoms such as tiredness, fatigue and exhaustion. The administration of iron reduces these symptoms of PMS, which affect many women monthly in mild to severe forms. Iron is also a cofactor of the enzyme tryptophan hydroxylase, which catalyzes the conversion of tryptophan to serotonin precursor 5-hydroxytryptophan (5-HTP). Low iron levels have been associated with postnatal depression, a disorder associated with hypersensitivity to fluctuations in ovarian hormones. In recent studies, high doses of non-haem iron, mostly of plant origin, have been associated with a lower risk of PMS. Therefore, a daily intake of plant iron is recommended to prevent premenstrual symptoms such as fatigue and exhaustion. Ginkgo biloba, a plant originating in China, where it has been used for hundreds of years in Traditional Chinese Medicine (TCM), is particularly rich in active ingredients such as flavonoid glycosides and terpene lactones. With very good tolerance and safety, the plant extract has been shown to have a beneficial effect on symptoms of premenstrual syndrome. In a study the use The patented Pinus Pinaster extract Pycnogenol® contains polyphenols from a standardized pure substance extract obtained from the bark of the maritime pine (Pinus pinaster) and grape seeds. In addition to inhibiting cyclooxygenase, pycnogenol® can reduce the activity of proinflammatory proteins such as NF-kB (12) and C-reactive protein and thus influence inflammatory processes in the body. In several studies of women with dysmenorrhea, the intake of pycnogenol® resulted in a significant reduction in menstrual pain. An estrogen-induced increase in prostaglandin levels is a common cause of lower abdominal pain during menstruation. A clinical study in 116 women with dysmenorrhea demonstrated the pain-reducing effect of pycnogenol® during menstruation. Pain intensity and duration were significantly reduced, leading to a reduction of up to 50% in the use of non-steroidal painkillers. Monk pepper (Vitex agnus-castus) is a traditional and very popular remedy for gynecological complaints, especially in the Anglo-American and European region. Since conventional PMS treatments with hormones and synthetic antidepressants are not well accepted, monk pepper extract is sometimes used. The popularity of complementary/alternative therapies has increased in recent years and these treatments have been used more frequently by women (48.9 %) than by men (37.8 %). As early as 2011, a study confirmed the effect of Vitex agnus-castus on the most common symptom of menopause, hot flushes. In 2012, a study reviewed 13 randomized controlled trials on the use of Vitex agnus-castusVitex for PMS, PMDS and hyperprolactinemia and concluded that the plant was beneficial and well tolerated in the treatment of all three disorders. In a placebo-controlled study, 20 mg Vitex-agnus-castus extract was determined to be the optimal dose for the treatment of PMS symptoms. The extract significantly reduces PMS symptoms such as irritability, mood swings, anger, headache, bloating and breast tenderness, as well as water retention, cravings and irritability. It is also very well tolerated and has shown mild, temporary side-effects in only in a few case. The effect of Vitex agnus-castus on migraine sufferers with premenstrual syndrome has also been demonstrated. Of 107 women, 66 reported a dramatic reduction in PMS symptoms, 26 a slight reduction and 8 no effect. Additionally, 42 % of the patients had half as many migraine attacks and 57 % of the patients had half as many headaches per month on half as many days. No patient suffered from significant side effects. |